
Organ Recovery
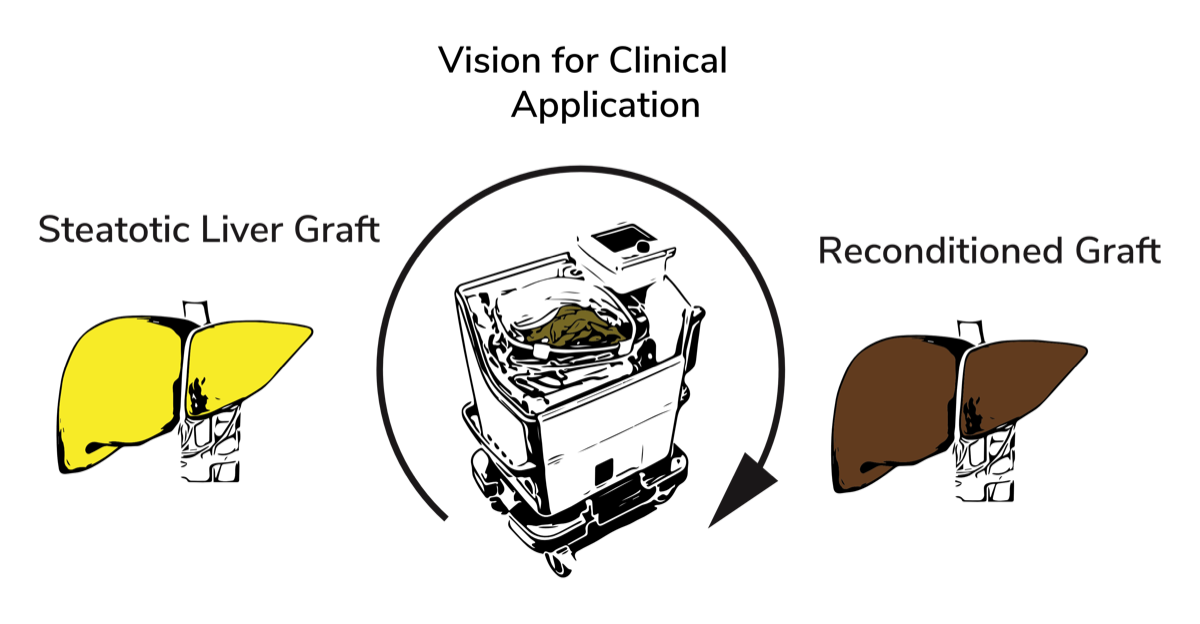
Background
We outline the current problem in our publication Prevalence of Steatosis Hepatis in the Eurotransplant Region: Impact on Graft Acceptance Rates.
Normothermic Extracorporeal Liver Machine Perfusion
Liver machine perfusion was initially considered in the earlier years of transplantation for organ preservation but rediscovered within the last years as concept to improve the quality of marginal grafts. Clinically applicable machine perfusion concepts for the liver mainly differ in regard to their perfusion temperature:
In hypothermic (HMP) or subnormothermic machine perfusion (SNMP), the liver graft is perfused at temperatures ranging from 1 – 21 °C. Under these conditions, the increased solubility of oxygen facilitates the use of perfusate solutions without oxygen carriers. HMP of liver grafts is currently under clinical evaluation: Guarrera et al. showed less early graft dysfunction and lower enzyme release after end-ischemic hypothermic machine perfusion of livers from brain-dead donors (DBD) compared to static cold preservation. Dutkowski et al. performed hypothermic oxygenated machine perfusion (HOPE) of DCD liver grafts and showed that it was effective against reperfusion injury. Hoyer et al. recently reported a clinical series of machine-assisted slow controlled oxygenated rewarming of cold-stored DBD livers, resulting in 50% reduction of the peak serum transaminases after transplantation compared to untreated controls.
Normothermic machine perfusion (NMP) at 37°C, in contrast to perfusion at lower temperatures, necessitates the use of oxygen carriers, mainly red blood cells . NMP maintains the graft in a near-to-physiological state, which avoids the depletion of cellular energy and accumulation of waste products, and thus minimizes the preservation injury. Ravikumar et al. and Selzner et al. recently demonstrated the safety and feasibility of NMP in phase 1 clinical trials in Europe and North America. A phase 3 randomized controlled clinical trial is currently being performed to compared NMP to static cold storage.
PD Dr. Raschzok and his team have established a lab-scaled, portovenous murine liver perfusion system similar to the setup described by Tolboom et al. The perfusion system consists of a pressure-controlled roller pump, an oxygenator and a custom-made perfusion chamber. As perfusate, Dulbecco's Modified Eagle´s Medium (DMEM) substituted with rat erythrocytes, rat plasma and HEPEs buffer was used. Heparin was continuously infused into the perfusate.
-
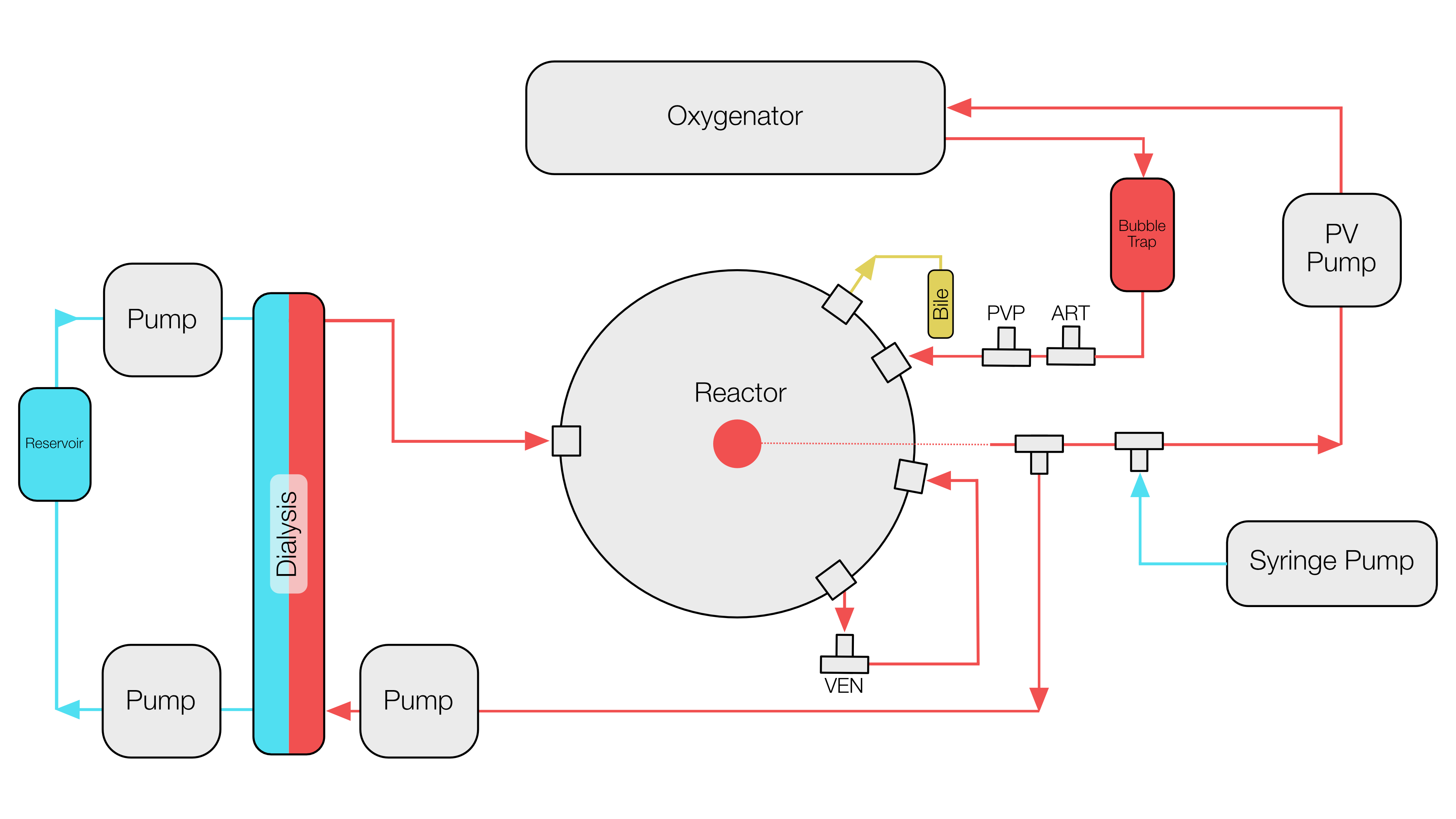 Schematic of the machine perfusion system
Schematic of the machine perfusion system -
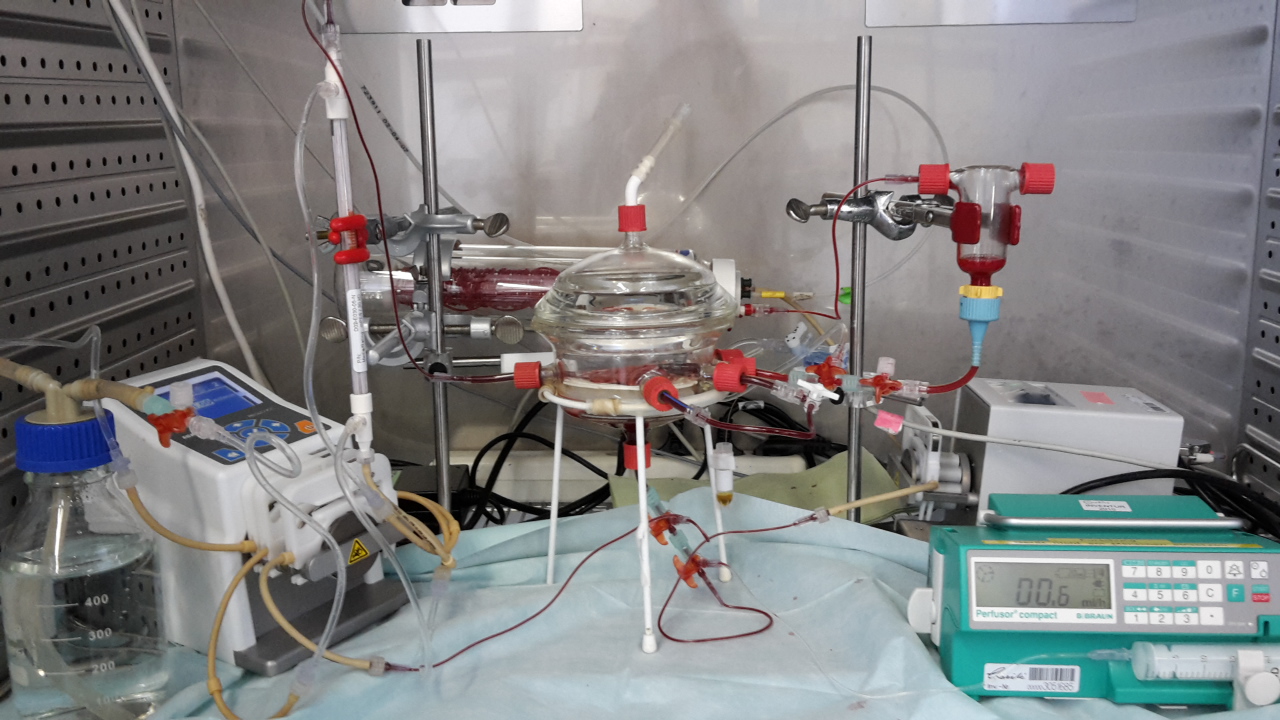 Perfusion system during an experiment
Perfusion system during an experiment -
 Setting up an experiment
Setting up an experiment
The addition of erythrocytes led to significantly lower transaminase secretion but to potassium excess >14 mmol/L in the perfusate. The inclusion of a miniaturized oxygenator, a dialysis circuit, the decrease of the perfusate from 100 to 50ml, and the increase of the hematocrit from 7 to 15% resulted in significantly lower transaminase secretion , normal potassium levels and a preserved liver architecture in Hematoxylin & Eosin (H&E) staining after 6 hours of perfusion.
First results can be found in Improvement of normothermic ex vivo machine perfusion of rat liver grafts by dialysis and Kupffer Cell inhibition with glycine which was published in Liver Transplantation.
-
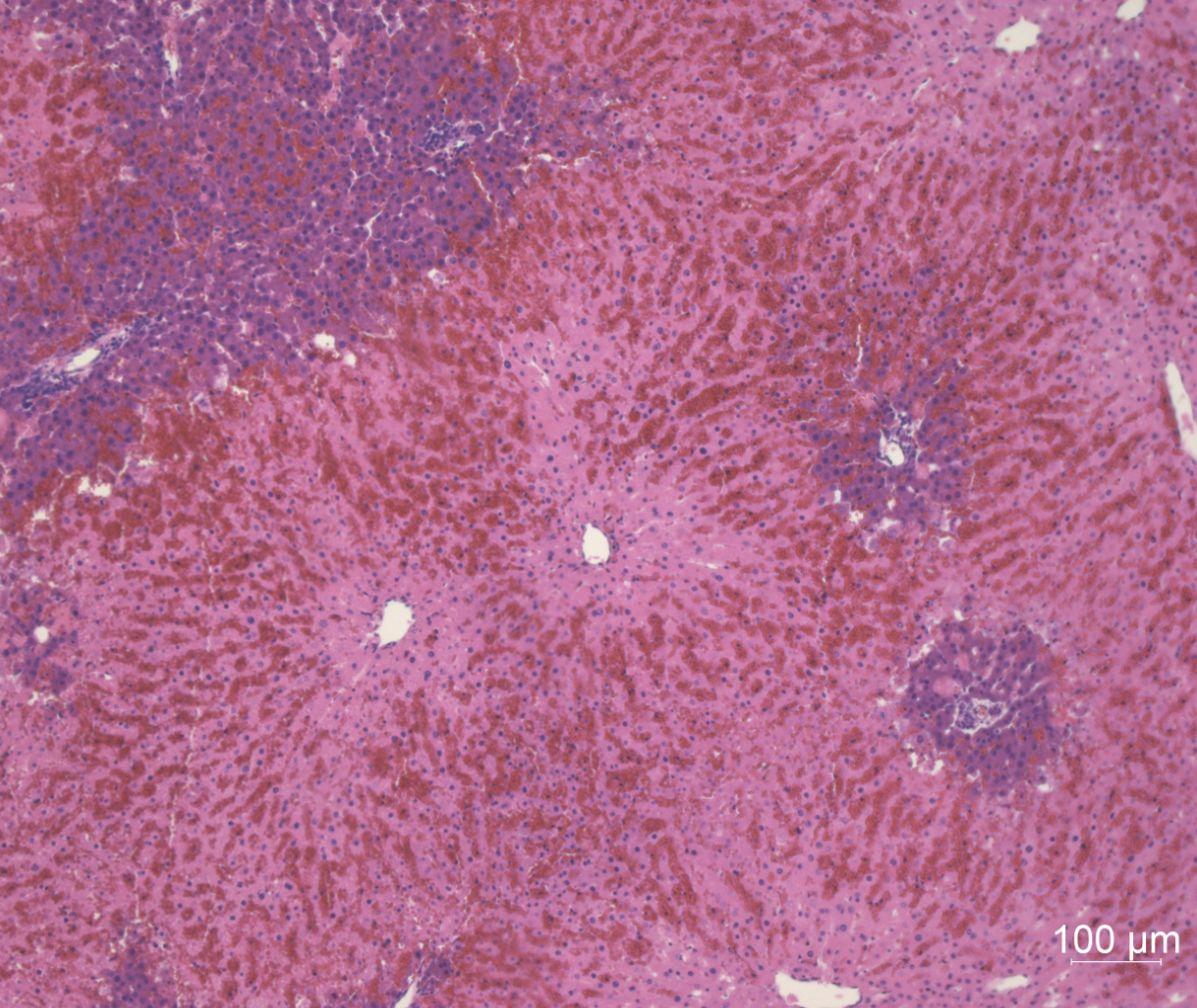 Rat Liver | H&E | 100x | First trials with high rates of necrosis
Rat Liver | H&E | 100x | First trials with high rates of necrosis -
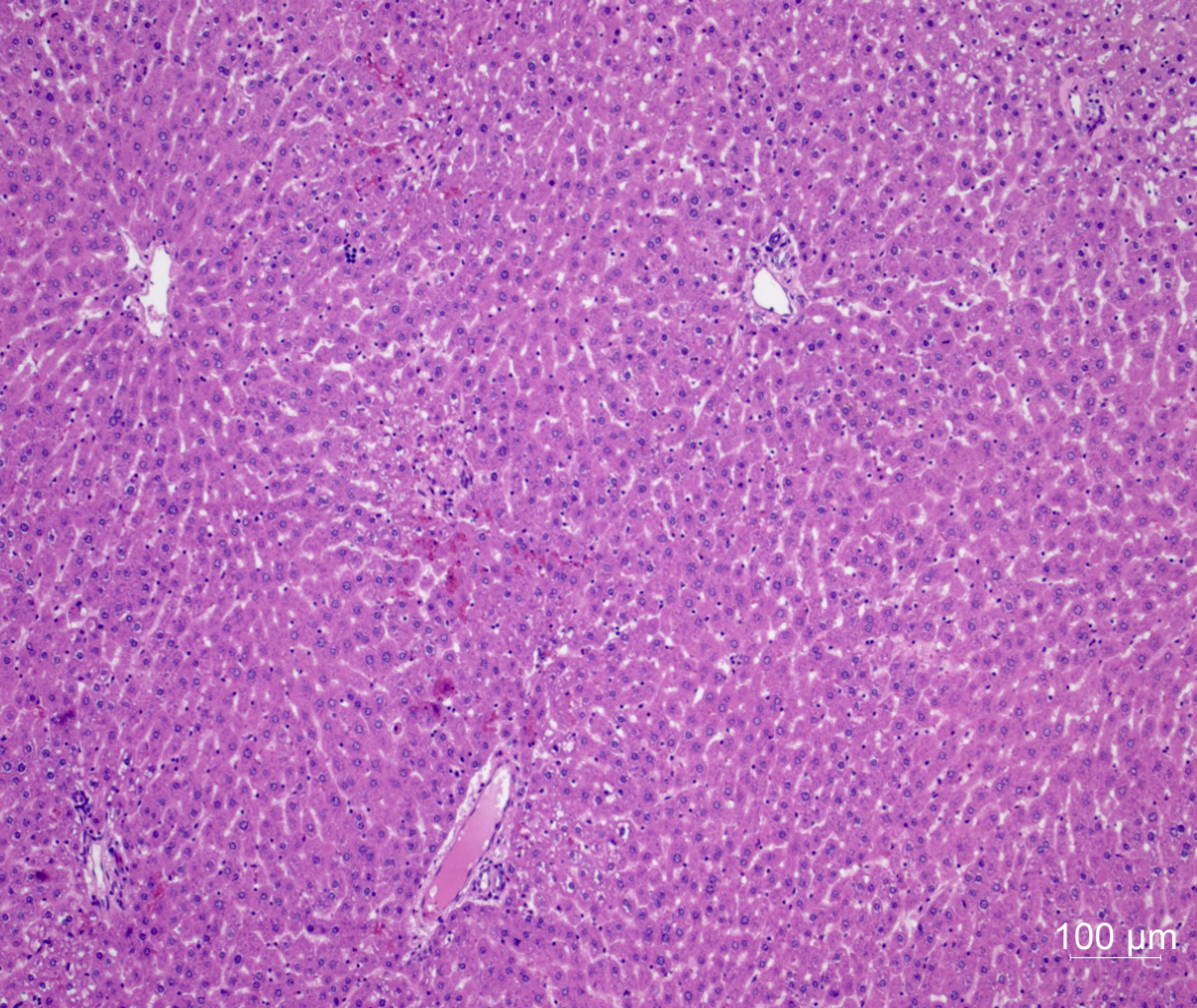 Rat Liver | H&E | 100x | Improved perfusion system
Rat Liver | H&E | 100x | Improved perfusion system
Our Team





Johannes Bornemann
Student

Leonard Boerger
Student

Linda Gilles
Student

Marie Kröhn
Doctoral Student

Julian Michelotto
Student

Vanessa Muth
Student

Anna Pietsch
Student

Nathalie Roschke
Student

Maximilian Zimmer
Student

Luca Padoan
Student

Kilian Walter
Student

Alessia Santamaria
Doctoral Student

Vincent Appel
Student